






























Calculous prostatitis– complications of chronic inflammation of the prostate gland, characterized by the formation of stones in the acini or excretory ducts of the gland. Calculus prostatitis is accompanied by increased urination, dull pain in the lower abdomen and perineum, erectile dysfunction, the presence of blood in the seminal fluid, and prostatorrhea. Calculous prostatitis can be diagnosed using digital examination of the prostate, ultrasound of the prostate gland, urographic examination, and laboratory examinations. Conservative therapy for calculous prostatitis is carried out with the help of drugs, herbal remedies, and physiotherapy; If these measures are ineffective, stone destruction with a low-intensity laser or surgical removal is indicated.
General information
Calculus prostatitis is a form of chronic prostatitis, accompanied by the formation of stones (prostatoliths). Calculus prostatitis is the most common complication of the long-term inflammatory process in the prostate gland, which should be addressed by specialists in the field of urology and andrology. During preventive ultrasound examinations, prostate stones are detected in 8. 4% of men of various ages. The first age peak in the incidence of calculous prostatitis occurs at the age of 30-39 years and is due to the increase in cases of chronic prostatitis caused by STDs (chlamydia, trichomoniasis, gonorrhea, ureaplasmosis, mycoplasmosis, etc. ). In men aged 40-59 years, calculous prostatitis, as a rule, develops against the background of prostate adenoma, and in patients over 60 years old it is associated with a decrease in sexual function.
The cause of prostatitis is calculus
Depending on the cause of formation, prostate stones can be true (primary) or false (secondary). Primary stones are initially formed directly in the acini and ducts of the gland, secondary stones migrate into the prostate from the upper urinary tract (kidneys, bladder or urethra) if the patient has urolithiasis.
The development of calculous prostatitis is caused by congestive and inflammatory changes in the prostate gland. Impaired emptying of the prostate gland due to BPH, irregular or lack of sexual activity, and a sedentary lifestyle. Against this background, the addition of moist infections to the genitourinary tract leads to blockage of the prostate duct and changes in the nature of prostate secretion. On the other hand, prostate stones also support chronic inflammatory processes and secretion stagnation in the prostate.
In addition to stagnation and inflammatory phenomena, urethro-prostatic reflux plays an important role in the development of calculous prostatitis - pathological reflux of a small amount of urine from the urethra into the prostate duct during urination. At the same time, the salt contained in the urine crystallizes, thickens and, over time, turns into stones. Causes of urethro-prostatic reflux can be narrowing of the urethra, trauma to the urethra, atony of the prostate and seminal tubercles, previous transurethral resection of the prostate gland, etc.
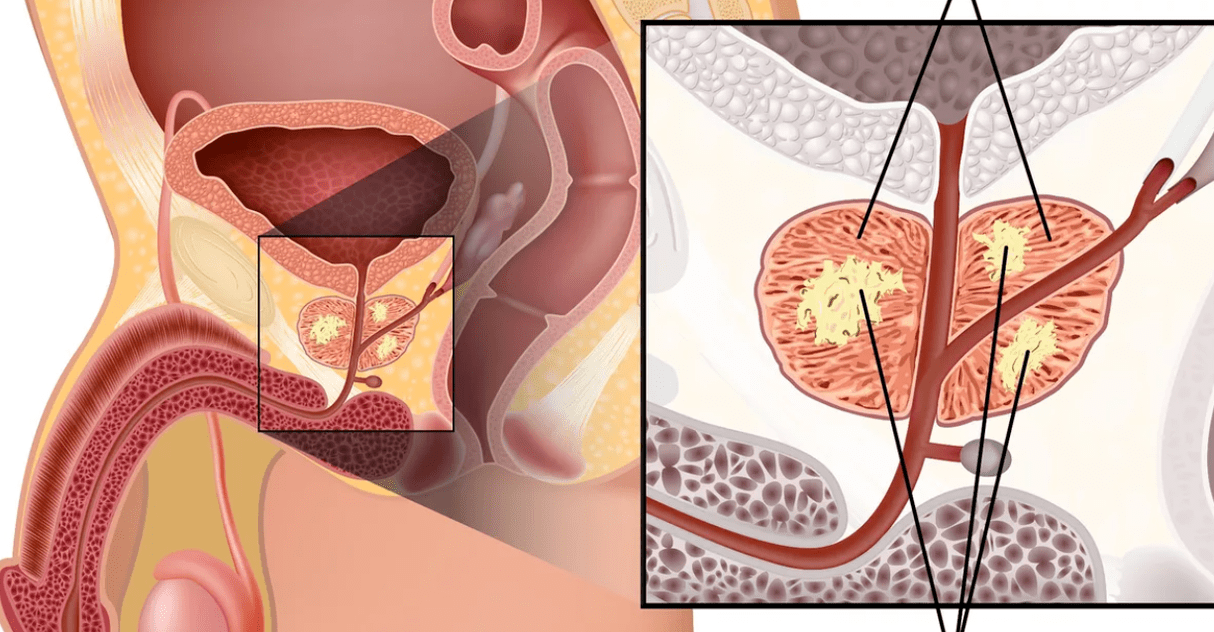
The morphological core for prostate calculus is amyloid bodies and desquamated epithelium, which gradually "grows" with phosphates and calcareous salts. Prostate stones are located in acini (lobules) that develop cystically or in the excretory duct. Prostatoliths are yellowish, spherical in shape, and vary in size (on average from 2. 5 to 4 mm); may be single or multiple. In terms of its chemical composition, prostate stones are the same as bladder stones. With prostatitis, calculi, oxalate, phosphate and urinary stones are most often formed.
Symptoms of calculous prostatitis
The clinical manifestations of calculous prostatitis generally resemble the chronic inflammatory process of the prostate. The main symptom in the clinic of calculus prostatitis is pain. The pain is dull, painful in nature; localized in the perineum, scrotum, above the pubis, sacrum or coccyx. Exacerbating painful attacks may be associated with defecation, sexual intercourse, physical activity, prolonged sitting on hard surfaces, long walks or bumpy driving. Calculous prostatitis is accompanied by frequent urination, sometimes with complete urinary retention; hematuria, prostatorrhea (leakage of prostate secretions), hemospermia. Characterized by decreased libido, weak erections, impaired ejaculation, and painful ejaculation.
Endogenous prostate stones can remain in the prostate gland for a long time without symptoms. However, a prolonged chronic inflammatory process and associated calculous prostatitis can lead to the formation of a prostate abscess, the development of vesiculitis, atrophy and sclerosis of glandular tissue.
Diagnosis of calculous prostatitis
To establish the diagnosis of calculous prostatitis, consultation with a urologist (andrologist), evaluation of existing complaints, and physical and instrumental examination of the patient is required. When performing a digital examination of the prostate rectum, a lumpy stone surface and a kind of crepitus are determined by palpation. Using transrectal ultrasound of the prostate gland, the stone is detected as a hyperechoic formation with a clear acoustic track; its location, quantity, size and structure are explained. Sometimes urography, CT and MRI of the prostate are used to detect prostatolith. Exogenous stones are diagnosed with pyelography, cystography and urethrography.
Instrumental examination of patients with calculous prostatitis is complemented by laboratory diagnostics: examination of prostate secretions, bacteriological culture of urethral discharge and urine, PCR examination for scraping for sexually transmitted infections, biochemical analysis of blood and urine, determination of prostate-specific antigen levels, sperm biochemistry, ejaculate culture, etc.
During examination, calcified prostatitis is differentiated from prostate adenoma, tuberculosis and prostate cancer, bacterial and chronic abacterial prostatitis. In calculous prostatitis that is not associated with prostate adenoma, the volume of the prostate gland and the PSA level remain normal.
Treatment of calculous prostatitis
Uncomplicated stones in combination with chronic inflammation of the prostate gland require conservative anti-inflammatory therapy. Treatment of calculous prostatitis includes antibiotic therapy, non-steroidal anti-inflammatory drugs, herbal drugs, physiotherapeutic procedures (magnetic therapy, ultrasound therapy, electrophoresis). In recent years, low-intensity lasers have been successfully used to destroy prostate stones non-invasively. Prostate massage for patients with calculous prostatitis is strictly prohibited.
Surgical treatment of calculous prostatitis is usually required in cases of complicated disease, its combination with prostate adenoma. When a prostate abscess is formed, the abscess is opened, and along with the outflow of pus, the passage of stones is also observed. Sometimes mobile exogenous stones can be pushed instrumentally into the bladder and subjected to lithotripsy. The removal of fixed stones of large size is performed in the process of the perineal or suprapubic part. When calculous prostatitis is combined with BPH, the optimal method of surgical treatment is adenomectomy, prostate TUR, prostatectomy.
Prognosis and prevention of calculous prostatitis
In most cases, the prognosis for conservative and surgical treatment of calculous prostatitis is favorable. Urinary fistula that does not heal in the long term can be a complication of prostate stone removal on the perineum. In the absence of treatment, the result of calculous prostatitis is the formation of abscesses and sclerosis of the prostate gland, urinary incontinence, impotence, and male infertility.
The most effective measure to prevent the formation of stones in the prostate gland is to contact a specialist when the first signs of prostatitis occur. An important role is for the prevention of STIs, the elimination of predisposing factors (uretro-prostatic reflux, metabolic disorders), age-appropriate physical and sexual activity. Preventive visits to a urologist and timely treatment of urolithiasis will help prevent the development of calculous prostatitis.